

NIH: A Monopoly On Human Health
NIH: A Monopoly On Human Health
Part 20: Doctors Proposed The Same Treatments That I Suggested In Dr. Fauci's Emails

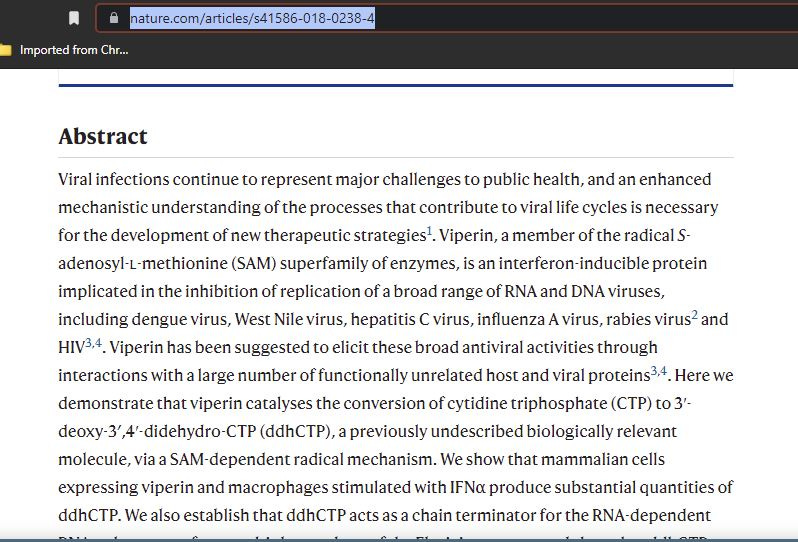
Early on during the Covid pandemic, I suggested several remedies that I thought could be simple cures. One of them was to use Ipratroprium Bromide Nasal Spray because it is an Anticholinergic. The other was to treat patients with an injection of Interferon a to prompt the body’s immune system to produce Viperin.
As many may not know, Dr. Fauci’s NIAID funds AAAAI, the National Allergy Bureau that measures pollen, mold, and seasonal allergy values in the air. During the beginning of covid, these values ceased to be reported, they were defunded for a time, and the NIAID’s name was scrubbed from their revised website. Some of the Cities haven’t reported since before covid. Some of the Cities have resumed reporting, but what’s interesting, is that during the time of the major spikes of covid infectivity, the mold spores were very high.
I was following this very closely for my own personal use because I am a sufferer of seasonal allergies that turns into bronchitis every year. I had been using the AAAAI tool before covid, so I knew what the normal routine was for reporting. High covid infectivity coincided with high mold count and high tree and grass pollen counts.
Even though AAAAI wasn’t reporting, I had printed some of the values and names of allergens from the years before so that I would know what I was more sensitive to, at what times. I found another site out of Ohio that was still reporting independently of AAAAI, so I could still get seasonal measurements even though it seemed that AAAAI had been conveniently shut down, defunded by NIAID, and their association to them removed. That seemed pretty conspicuous, and it made me curious.
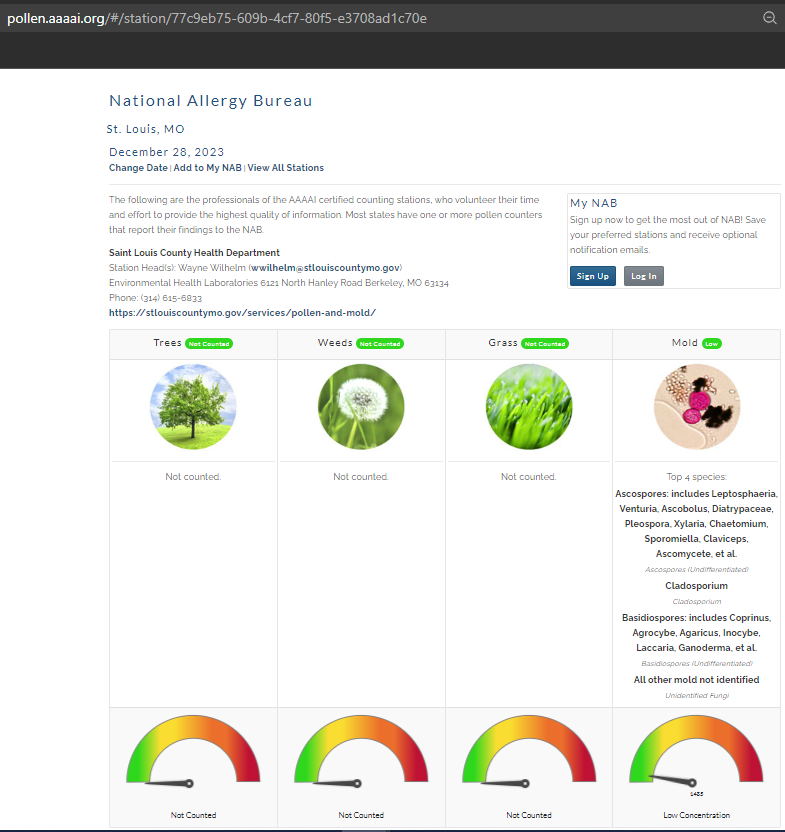
The earliest I could find after the beginning of covid that had resumed and that I had screenshotted was in July of 2021.
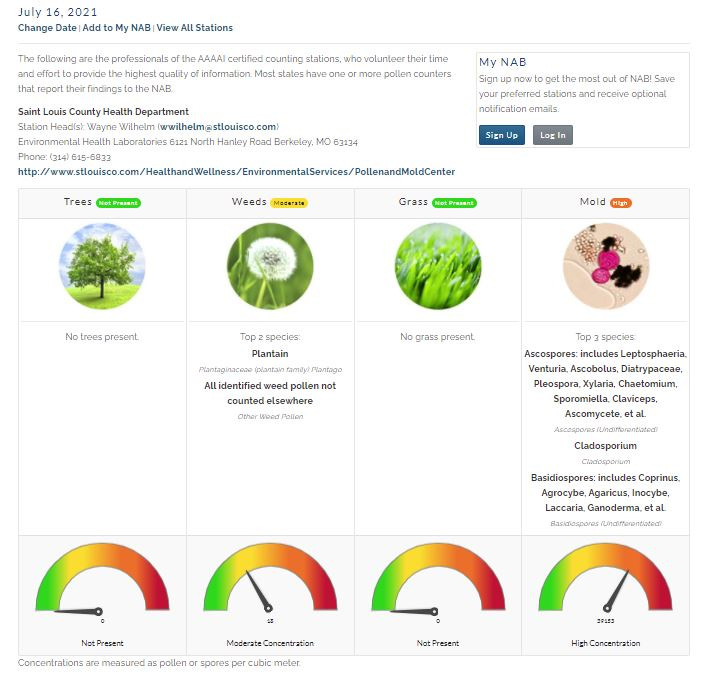
As you can see, there are similar mold species in July and December, the higher concentration being in July in comparison to the most recent St. Louis count for December 2023.

I had been prescribed Ipratroprium Bromide Nasal Spray for seasonal allergies. I worked in a Pharmacy for 10 years, so I knew that Ipratropruim Bromide was an Anticholinergic, that works on muscarinic acetylcholine receptors. I guess you have to know what an ACE Inhibitor is, but I did know that the ACE2 receptors were involved with covid, and that they play a role in the Renin-Angiotensin-Aldosterone Mechanism (System), which involves a protein and enzyme that results in Angiotensin I and II that is secreted from the top of the kidneys to control blood pressure and fluid and electrolyte balance.
The other receptors in the lung, which are the counterpart of muscarinic acetylcholine receptors, that act on ACE2 receptors are called nicotinic acetylcholine receptors, which could have been another avenue of treatment using Angiotensin II Receptor Blockers (ARB). Some other people thought so too.

Nicotinic receptors also play a role in tobacco use, but that’s another story as to why smokers faired better with regard to covid, because nicotine was occupying the space within the ACE2 neurotransmitter receptor.
Nicotinic acetylcholine receptors (nAChR) are widely distributed in neuronal and non-neuronal tissues, where they play diverse physiological roles. In this review, we highlight the recent findings regarding the role of nAChR in the respiratory tract with a special focus on the involvement of nAChR in the regulation of multiple processes in health and disease. We discuss the role of nAChR in mucociliary clearance, inflammation, and infection and in airway diseases such as asthma, chronic obstructive pulmonary disease, and cancer. The subtype diversity of nAChR enables differential regulation, making them a suitable pharmaceutical target in many diseases. The stimulation of the α3β4 nAChR could be beneficial in diseases accompanied by impaired mucociliary clearance, and the anti-inflammatory effect due to an α7 nAChR stimulation could alleviate symptoms in diseases with chronic inflammation such as chronic obstructive pulmonary disease and asthma, while the inhibition of the α5 nAChR could potentially be applied in non-small cell lung cancer treatment. However, while clinical studies targeting nAChR in the airways are still lacking, we suggest that more detailed research into this topic and possible pharmaceutical applications could represent a valuable tool to alleviate the symptoms of diverse airway diseases.
Beyond mold allergy reporting, Ipratroprium Bromide Nasal Spray, and Muscarinic and Nicotinic Acetylcholine Receptors, there was one more thing that I found that has been shown to alleviate all of the viruses that the NIH and WHO spend billions of tax dollars on to eradicate.
That something, is a naturally occurring substance produced by the Immune System of the body. An injection of Interferon alpha causes a series of actions that produce a substance known as Viperin. We always kept Interferon injections in the refrigerator in the Hospital Pharmacy, and it’s commonly on Hospital Formulary Drug Lists, which means they keep it in stock at all times.
It seems that on December 20, 2023, the NIH has a bulletin about Interferon alpha and beta. The bulletin says that it has been known to cure viruses such as Hepatitis B and C, but makes no recommendation to use it for hospitalized covid patients unless it’s in a Clinical Trial. That’s because they know it works, and the Hospital has it readily available. Also, they wanted to do us in with the covid protocol, the Remdesivir regimen, and the ventilator. They won’t give hospitalized patients monoclonal antibodies because you are a patient in the hospital. That’s the reason. You can’t make this stuff up! What other reason, besides knowing that it’s a natural cure, would they have to withhold it if not for a reason to justify globally dispersing all of that taxpayer grant money?
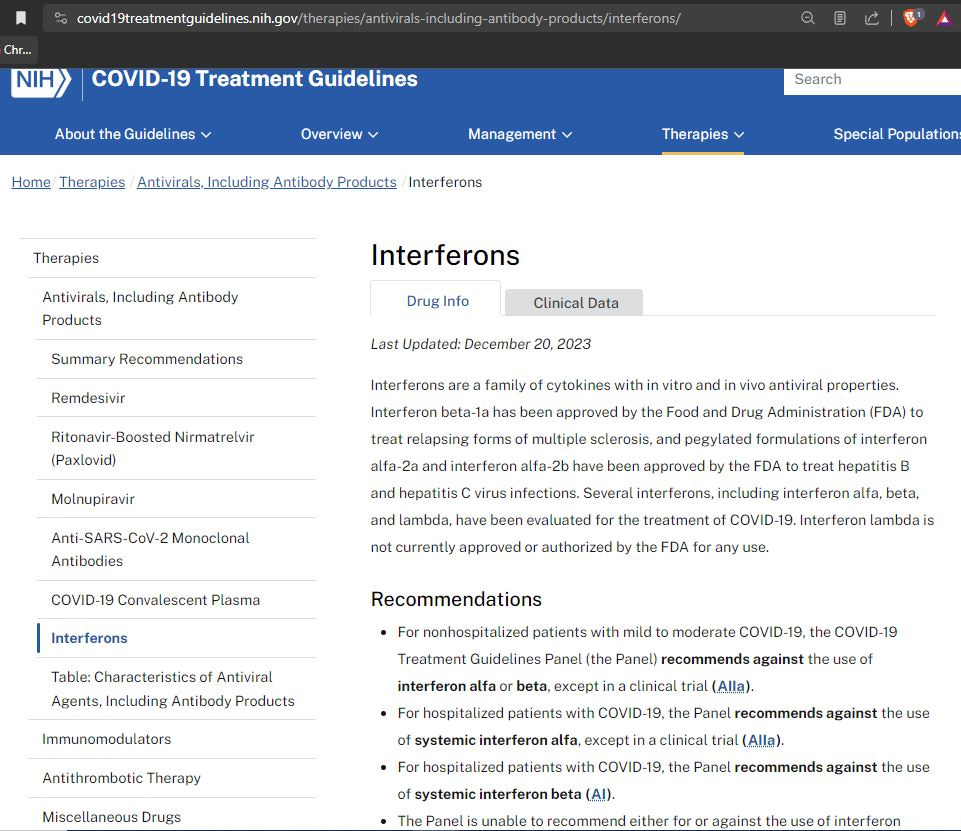
The covid Interferon alpha regimen rationale, (the one that works), is described like this:
Systemic interferon alfa and inhaled interferons have also been evaluated in patients with COVID-19. The trials that have evaluated the use of interferon alfa have generally been small or moderate in size and have not been adequately powered to assess whether this agent provides a clinical benefit for patients with COVID-19.6-8
They state that Interferon beta does not work, which gives a more documented rationale.
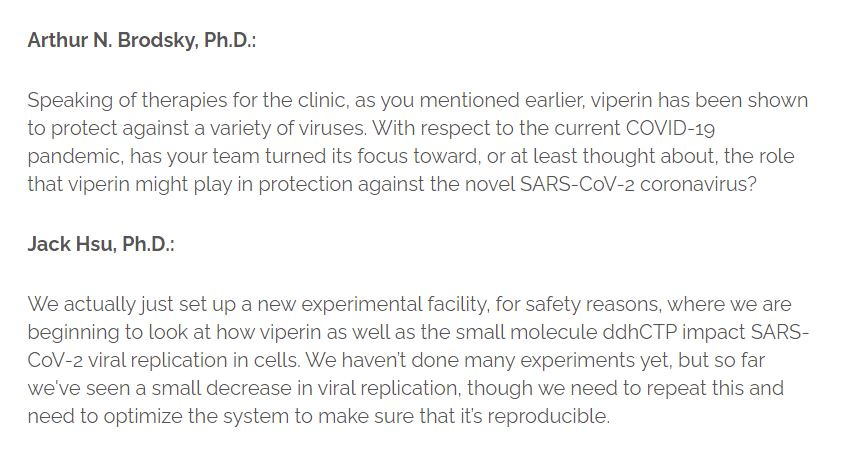
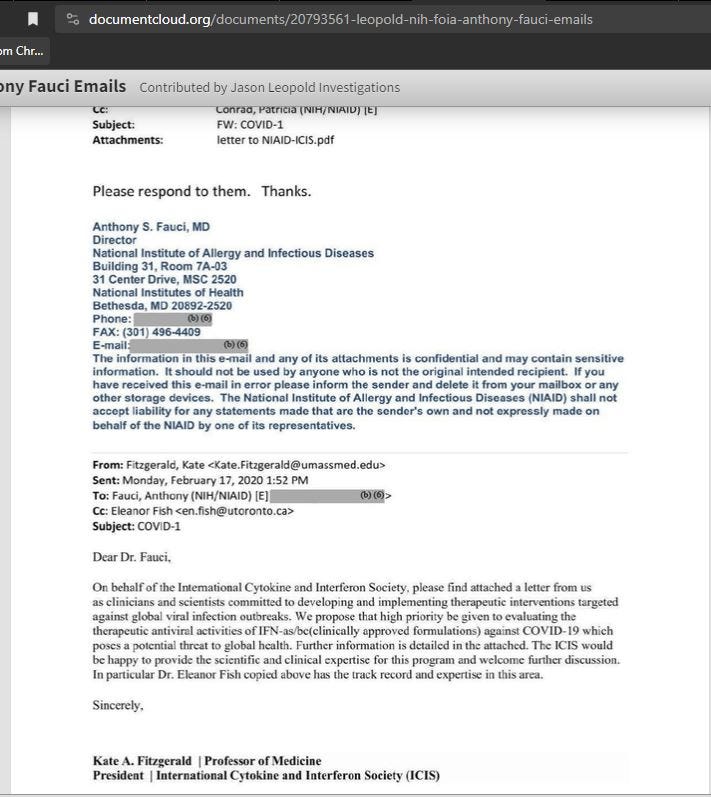
There were some other people besides myself who thought Interferon would be beneficial.
Benadryl works in the same way as Ipratroprium, and could have reduced secretions or potentially blocked receptors from foreign attachment.
Maybe giving Ipratroprium would have been counterproductive since it works on smooth muscle, but it is a bronchodilator, which seems like it could have been a good thing to do, but I’m no Doctor.